771
Views & Citations10
Likes & Shares
A study was undertaken to compare colistin
susceptibility using BMD and Vitek in carbapenem resistant gram negative
isolates to evaluate the discrepancies and further course of action.
Conclusion: The
broth micro dilution (BMD) technique is reliable and is easy to use method for
determining the MIC of Colistin. The results correlated with Vitek system
except for 2 isolates which showed very major errors which indicates that in
case of resistance to Colistin by Vitek, broth dilution method must be used for
correlation and to recheck the result. Also in case of Vitek system showing
susceptibility to Colistin, we can safely report those isolates without doing
micro broth dilution as we did not encounter any isolates which gave
susceptible on Vitek and resistant on micro broth dilution method.
Keywords:
Colistin, Vitek, Broth microdilution, MIC
INTRODUCTION
Colistin also
known as polymyxin E is an antibiotic produced by certain strains of the
bacteria Penibacillus polymyxa.
Colistin is a mixture of the cyclic polypeptides colistin A and B and belongs
to the class of polypeptide antibiotics known as polymyxins. Colistin is
effective against most Gram-negative bacilli.
Colistin is a
decades-old drug that fell out of favor in human medicine due to its kidney
toxicity. It remains one of the last-resort antibiotics for multidrug-resistant
Pseudomonas aeruginosa, Klebsiella pneumoniae and Acinetobacter
[1]. NDM-1 metallo-β-lactamase multidrug-resistant Enterobacteriaceae have also
shown susceptibility to colistin [2].
Colistin has been effective in treating
infections caused by Pseudomonas, Escherichia and Klebsiella species. Colistin
is an effective antibiotic for treatment of most multidrug-resistant
Gram-negative bacteria. It is used currently as a last-line drug for infections
due to severe Gram-negative bacteria followed by an increase in resistance
among Gram-negative bacteria.
Colistin resistance is
considered a serious problem, due to a lack of alternative antibiotics. Some
bacteria including Pseudomonas aeruginosa, Acinetobacter baumannii,
Enterobacteriaceae members, such as Escherichia coli and Klebsiella spp. have an acquired resistance against colistin.
Colistin is increasingly needed for the
treatment of infections caused by carbapenem-resistant Acinetobacter baumannii (CRAB) isolates [3]. The accurate
antimicrobial susceptibility testing (AST) of colistin is of obvious
importance; however, considerable discrepancies have been reported between the
available assays. To address this issue, EUCAST and CLSI recently formed a
Polymyxin.
Breakpoints Working
Group for colistin susceptibility testing [4], which recommended that broth
micro dilution (BMD), is the most valid method for colistin AST. Among the
diffusion methods, disc diffusion is unacceptable due to the large colistin
molecule, while several studies in the literature have reported considerable
discrepancies of the MICs produced by gradient tests [5]. The joint EUCAST/CLSI
working group recently confirmed the problems that both of the available
colistin gradient tests (manufactured by bioMe´rieux and Liofilchem) exhibit
[6]. Colistin has been traditionally
reported by all automated
STUDY
The broad objective of this study is to
explore the concept of mental health healing among pastors and possibilities of
collaboration with mental health professionals in Mzuzu.
Colistin susceptibility is done in our lab
using MICROLATESTR marketed by Transasia in India. It is a broth
micro dilution test which is CE=IVD approved for testing for Colistin. The cut
offs provide are 0.25, 0.5, 1.0, 2.0, 4.0, 8.0 and 16.0 mcg/ml.
Breakpoints for Colistin to
test Pseudomonas spp. and Acinetobacter spp. are as follows as per
CLSI 2018. Resistant: >=4 mcg/ml, Susceptible: <=2 mcg/ml.
Breakpoints for Colistin to
test Pseudomonas spp. and Acinetobacter spp. are as follows as per
CLSI 2018. Resistant: >=4 mcg/ml, Susceptible: <=2 mcg/ml.
Breakpoints for Colistin to
test Enterobactericeae are as follows as per EUCAST 2019. Resistant: >=2
mcg/ml, Susceptible: <=2 mcg/ml.
We have followed EUCAST for
Enterobactericeae and CLSI for Pseudomonas
spp. and Acinetobacter spp. Recommendations
for MIC determination of colistin (polymyxin E).
As recommended by
the joint CLSI-EUCAST Polymyxin Breakpoints Working Group published at http://www.eucast.org on 22 March, 2016 [4,7].
Colistin (polymyxin E) MIC determination is
associated by several methodological issues. The issues have been extensively
investigated by the CLSI-EUCAST joint Polymyxin Breakpoints Working Group and
the following method for determination of colistin MIC was agreed:
1. Reference
testing of Enterobacteriaceae, Pseudomonas aeruginosa and Acinetobacter
spp. is by the ISO-standard broth micro dilution method (20776-1).
Note:
a. Cation-adjusted
Mueller-Hinton Broth is used.
b. No
additives may be included in any part of the testing process (in particular, no
polysorbate-80 or other surfactants).
c.
Trays must be made of plain polystyrene
and not treated in any way before use.
d. Sulphate
salts of polymyxins must be used (the methane sulfonate derivative of colistin
must not be used - it is an inactive pro-drug that breaks down slowly in
solution).
2. Susceptibility testing by other methods,
including agar dilution, disk diffusion and gradient diffusion, cannot be
recommended until historical data have been reviewed or new study data have
been generated. Work on these methods is ongoing.
RESULTS
A total of 90 isolates over the 2 months were
studied (July-August 2019). All the isolates were carbapenem resistant Pseudomonas aeruginosa, Acinetobacter
baumannii and Enterobactericieae.
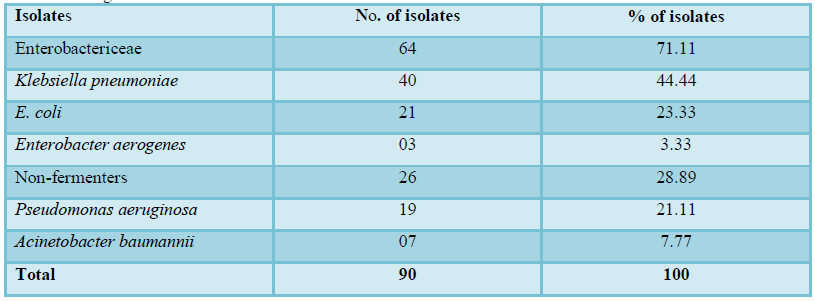
The carbapenem resistant isolate distribution
was as follows:
1. Carbapenem
resistant Enterobactericeae are
a majority of the isolates which
comprises of 71.11% of all the isolates.
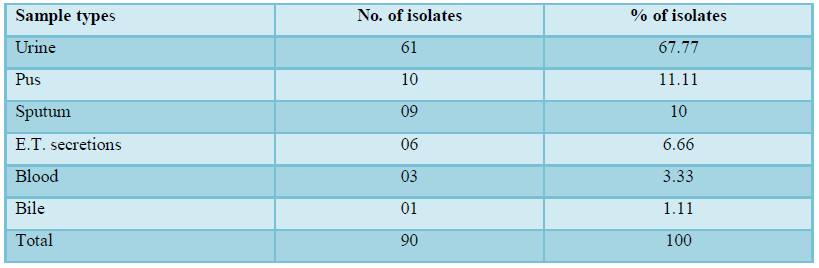
2. The
sample distribution for carbapenem resistant gram negative isolates is as
follows:
3. Urine forms the bulk of samples with carbapenem resistant gram negative isolates (67.77%).
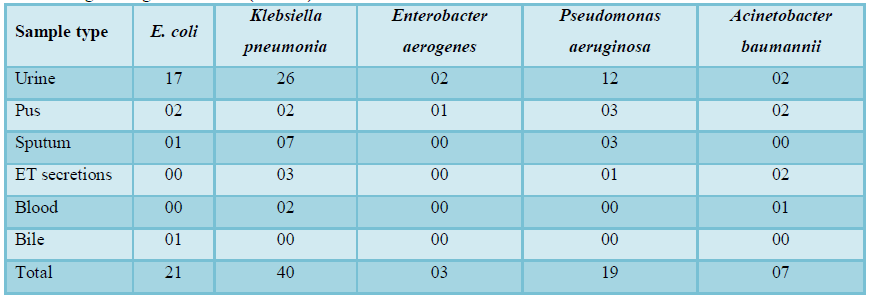
The organism distribution sample wise is as
follows:
4. Klebsiella
causing UTI is the predominant isolate-sample wise followed by E. coli and Pseudomonas in urine.
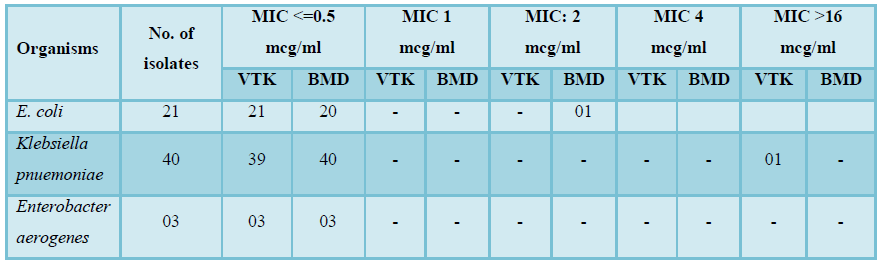
MIC
distribution in gram negatives by BMD is as follows:
5. 1 out
of 21
E. coli isolates showed discrepancy, and 1 out of 40 Klebsiella pneumoniae isolates showed
discrepancy. 3 Enterobacter isolates showed no discrepancy.
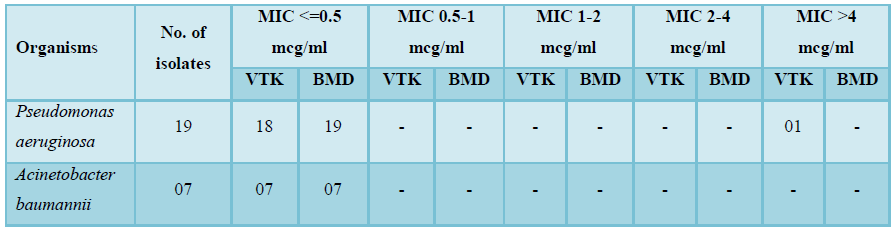
6.
1 Pseudomonas isolate showed MIC
discrepancy resulting in major error in interpretation. 7 isolates showed minor
difference in MIC values.
Details
of the discrepancy:
a. a. Minor
discrepancy is when there are differences in MIC values obtained by both the
methods but no change in category of interpretation.
b. b. Major
discrepancy is when difference in MIC values cause difference in category of
interpretation.
DISCUSSION
1. Carbapenem
resistant Enterobactericeae are a majority of the isolates. Klebsiella (28.88%)
causing UTI is the predominant isolate-sample wise followed by E. coli (18.88%) and Pseudmonas (13.33%)
in urine. Study carried out by Marya et al. [8] showed similar findings of
Klebsiella being the predominant isolate.
2. Urine forms the bulk of samples with carbapenem resistant gram negative isolates (67.77%). Study by Marya et al. [8] showed similar findings of UTI contributing to carbapenem resistant isolates.
3. In case of Klebsiella pneumoniae out of 40 isolates in our study, only 1 isolate had a discrepancy in MIC values and the MIC given by Vitek was >=16 mcg/ml. We infer that in case of Klebsiella pneumoniae, reconfirmation by BMD needs to be done only in case of MIC >=16 mcg/ml. More number of isolates will have to be studied to corroborate the above inference.
4. In
case of Enterobacter aerogenes, only
3 isolates were studied and had no discrepancy. But the low number of isolates
does not allow any conclusion to be made.
5. In
case of E. coli, out of 20 isolates,
3 had discrepancy in the values of MIC, which was minor error as it did not
change the category of interpretation. So reporting by Vitek 2 compact for them
can be taken into consideration.
6. In
case of Acinetobacter, 7 isolates were studied and had no discrepancies. Yen et
al. [9] showed similar findings.
7. But
because the outcome of colistin use is dependent on the exact value of colistin
MIC, this testing will have to be continued.
8. Our
study is limited by the fact that we do not have a single case of colistin
resistance by BMD. We did not find any such study.
CONCLUSION
1. The broth micro dilution (BMD) technique is reliable and is easy to use method for determining the MIC of Colistin. The results correlated with Vitek 2 compact except for 2 isolates which showed very major errors which indicates that in case of resistance to Colistin by Vitek, broth dilution method must be used for correlation and to recheck the result.
2. Also in case of Vitek 2 Compact showing susceptibility to Colistin, we can safely report those isolates without doing micro broth dilution as we did not encounter any isolates which gave susceptible on Vitek and resistant on micro broth dilution method.
REFERENCES
1. Falagas ME, Grammatikos AP,
Michalopoulos A (2008) Potential of old-generation antibiotics to address
current need for new antibiotics. Expert Rev Anti-infect Ther 6: 593-600.
2. Polymyxin E (2016) Colistin - The
antimicrobial index knowledge base - TOKU-E. Retrieved 28 May 2016.
3. Karaiskos I, Giamarellou H (2014)
Multidrug-resistant and extensively drug resistant Gram-negative pathogens:
Current and emerging therapeutic approaches. Expert Opin Pharmacother 15:
1351-1370.
4. EUCAST (2016) Recommendations for
Colistin (Polymyxin E) MIC Testing-Joint EUCAST and CLSI Recommendation.
5. Dafopoulou K, Zarkotou O,
Dimitroulia E (2015) Comparative evaluation of colistin susceptibility testing
methods among carbapenem-non-susceptible Klebsiella
pneumoniae and Acinetobacter
baumannii clinical isolates. Antimicrob Agents Chemother 59: 4625-4630.
6. EUCAST (2016) EUCAST Warnings
Concerning Antimicrobial Susceptibility Testing Products or
Procedures—Antimicrobial Susceptibility Testing of Colistin—Problems Detected
with Several Commercially Available Products.
7. Alexander LE, Loutit J, Tumbarello
M, Wunderink R, Felton T, et al. (2017) Carbapenem-resistant Enterobacteriaceae
infections: Results from a retrospective series and implications for the design
of prospective clinical trials. Open Forum Infect Dis 4.
8. Zilberberg DM, Nathanson HB,
Sulham K, Fan W, Shorr AF (2017) Carbapenem resistance, inappropriate empiric
treatment and outcomes among patients hospitalized with Enterobacteriaceae
urinary tract infection, pneumonia and sepsis. BMC Infect Dis 17: 279.
9. Yen T, Lily T, Ng SY, Poh K (2007)
Susceptibility testing of unconventional antibiotics against multi resistant Acinetobacter spp. by agar dilution and
Vitek 2. Diagn Microbiol Infect Dis 58: 357-361.
-
 Table 1
Table 1 -
Table 2
-
Table 3
-
Table 4
-
Table 5
-
Table 6

QUICK LINKS
- SUBMIT MANUSCRIPT
- RECOMMEND THE JOURNAL
-
SUBSCRIBE FOR ALERTS
RELATED JOURNALS
- Journal of Neurosurgery Imaging and Techniques (ISSN:2473-1943)
- Journal of Blood Transfusions and Diseases (ISSN:2641-4023)
- Journal of Allergy Research (ISSN:2642-326X)
- Journal of Psychiatry and Psychology Research (ISSN:2640-6136)
- Journal of Oral Health and Dentistry (ISSN: 2638-499X)
- Journal of Cancer Science and Treatment (ISSN:2641-7472)
- Archive of Obstetrics Gynecology and Reproductive Medicine (ISSN:2640-2297)


